Medication Management
What guidance does the Nursing and Midwifery Board of Ireland provide regarding the safe and professional management of medications?
Can I administer vaccinations as a registered nurse or midwife?
Yes, you may administer vaccinations if this is within your individual scope of practice.
As a regulated professional, you are accountable for your decisions and for the outcomes of the care you provide, regardless of your role, work setting, or whether you are working under direction or as part of a team. You must use the Code to guide your professional judgement and decision making, including decisions about your scope of practice.
Scope of practice refers to what a registered nurse or registered midwife can safely and appropriately do. It is informed by education, current competence, authority, division(s) of the Register, and the population you are registered to care for.
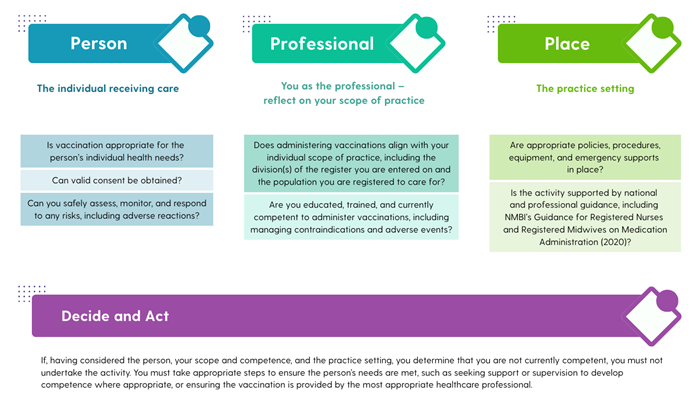
A practical way to support professional judgement in relation to the administration of vaccinations is to use the NMBI Decision Making Framework outlined in the Code. The framework provides a structured approach to ethical and professional decision making by considering the individual, the professional, and the practice setting.
When deciding whether to administer vaccinations, you should consider:
Registrants should also have regard to relevant national and professional guidance that supports safe vaccination practice, including:
Vaccination scope: Key reminders
- You may only administer vaccinations if this is within your individual scope of practice.
- Your scope of practice is informed by your education, current competence, division(s) of the Register, authorisation, and the population you are registered to care for, in line with the Code.
- Always apply the NMBI Decision Making Framework by considering the individual receiving care, you as the professional, and the practice setting.
- Being asked, directed, or expected by an employer to administer a vaccine does not extend your scope of practice.
- You must be currently competent to administer vaccinations safely, including assessing suitability, obtaining consent, monitoring for adverse reactions, and responding to emergencies.
- Vaccination practice must be supported by appropriate policies, procedures, equipment, and clinical governance arrangements.
- You must practise in line with NMBI’s Guidance for Registered Nurses and Midwives on Medication Administration (2020) and relevant national immunisation guidance.
- If administering vaccinations is outside your scope or competence, you must not proceed and must ensure the person receives care from the most appropriate healthcare professional.
- You are personally accountable for your decisions, actions, omissions, and the outcomes of care provided, in line with the Code.
Can I administer vaccinations as a nurse/midwife when there is no doctor on site?
You may administer vaccinations in the absence of a doctor where this is within your individual scope of practice and with regard to professional and national guidance documents. There is no requirement in legislation or in NMBI standards for a doctor to be physically present when a registered nurse or registered midwife administers a vaccine.
Scope of practice means that:
- You have the appropriate education, training, and current competence to administer the vaccine safely, including the ability to assess, monitor, and respond to risks such as adverse reactions.
- The practice setting has appropriate policies, procedures, protocols, and clinical governance arrangements in place.
- The activity is carried out in accordance with the Code of Professional Conduct and Ethics for Registered Nurses and Registered Midwives, including the Scope of Practice and Professional Guidance (NMBI, 2025) and NMBI’s Guidance for Registered Nurses and Registered Midwives on Medication Administration (2020).
In line with the Code, registered nurses and registered midwives are personally accountable for their professional practice, including their decisions, actions, omissions, and the outcomes arising from the administration of vaccinations. You must ensure that care is delivered safely and in line with the needs, rights, and wishes of the individual receiving the vaccine.
Can a registered midwife administer childhood vaccinations in a GP practice?
No. The scope of practice of a registered midwife includes care during the antenatal, intranatal, and postnatal periods, with the postnatal period defined as up to six weeks following delivery. As primary childhood immunisation schedules generally begin at eight weeks, administering these vaccinations falls outside the scope of midwifery practice.
Scope of practice refers to what a registered nurse or registered midwife can safely and appropriately do, in line with the Code. It is informed by your education, current competence, authority, division(s) of the Register and the population you are registered to care for.
Working in a GP practice or being asked by an employer to carry out a task does not extend scope of practice. If an activity is outside their scope, a midwife must not carry it out and should refer to an appropriate healthcare professional.
As a regulated professional, you are accountable for your decisions and for the outcomes of the care you provide, regardless of your role, work setting, or whether you are working under direction or as part of a team.
Are registered nurses and midwives required by NMBI to double-check medications as part of their role in administering medications?
No. There is no legal or NMBI requirement that medications must be double checked as part of the nurse or midwife’s role in medication administration.
It is first helpful to clarify what is meant by double checking. An independent double check, sometimes referred to as independent verification, involves one nurse or midwife carrying out their own calculation or check of the medication and then comparing this with a colleague. This is a safety measure, not a regulatory requirement.
NMBI recognises that there are many practice settings where a nurse or midwife may be working alone, such as in community settings, residential care units, or during night duty. In these circumstances, it is not always possible to carry out a double check, and the absence of an independent verifier does not in itself prevent medication administration.
For patient safety and risk management purposes, health service providers may require double checking of certain medicines as per local policies, procedures, protocols, and guidelines. This may particularly be the case for medicines considered high risk or high alert, or where complex calculations are required. These requirements are determined at organisational level, not by NMBI or legislation.
As with all medication administration, professional accountability rests with the nurse or midwife administering the medicine. You must apply professional judgement, practise within your individual scope of practice, and administer medicines safely in line with medicines legislation, NMBI guidance, and local policy, regardless of whether an independent verifier is involved or not.
Can a nursing or midwifery student act as a cosigner for MDA Schedule 2 drug checks, or is this role limited to me as a registered nurse or midwife?
A nursing or midwifery student may act as a second checker where this is permitted by local policy and it is appropriate to their level of education and competence, as assessed by their supervisor. Where a student is involved, the registrant as the regulated professional remains accountable for ensuring that medicines are checked and administered safely and in line with the Code, medicines legislation, and NMBI guidance.
All registered nurses and registered midwives must practise medication management in line with the Code, relevant medicines legislation, and regulatory guidance on medication management, including:
As a regulated professional, you are accountable for the safe preparation, checking, and administration of medicines, including controlled drugs. This must be carried out within your individual scope of practice, which is informed by your education, current competence, authority, division(s) of the Register, and the population you are registered to care for.
A two person check for medicines administration, including controlled drugs, is an organisational requirement as part of safe medication management and not a legal one. One of the individuals involved in checking medication administration must be a registered nurse or midwife, and decisions about who may act as the second checker are determined by local policy.
Can a medication protocol be used to support person-centred, timely care?
Yes. A medication protocol may be used by a healthcare organisation to support person centred, timely, and safe care, where it is developed and implemented in line with NMBI’s Guidance to Nurses and Midwives on Medication Management (2007). This guidance sets out the regulatory expectations for medication protocols and supports their use to authorise nurses and midwives to supply and administer specified medicines to defined groups of individuals in clearly identified clinical circumstances, where supported by local policy.
Medication protocols must be developed and governed appropriately. This includes evidence based development, multidisciplinary oversight, clearly defined inclusion and exclusion criteria, transparent accountability arrangements, and regular monitoring, audit, and review, as outlined in the 2007 guidance.
When working under a medication protocol, you must practise within your individual scope of practice and continue to exercise professional judgement. The use of a protocol does not replace professional judgement or remove responsibility for safe care. In line with the Code, you remain personally accountable for your decisions, actions, and the outcomes of care.
The Code of Professional Conduct and Ethics for Registered Nurses and Registered Midwives (NMBI, 2025) reinforces that care must be person centred, respecting the individual’s rights, values, preferences, and expressed wishes. Nurses and midwives are required to support individuals to participate in decisions about their care and to ensure that care is delivered safely, ethically, and in accordance with professional standards.
When appropriately designed and governed, a medication protocol can support timely responses to assessed needs and facilitate access to treatment, while maintaining person centred decision making and full professional accountability for the care provided.
Can a Registered Nurse Prescriber prescribe a Schedule 2 MDA drug such as methylphenidate?
Yes. Registered Nurse Prescribers (RNPs) and Registered Midwife Prescribers (RMPs) may prescribe certain controlled drugs, including some Schedule 2 MDA medicines such as methylphenidate, where this is explicitly permitted under medicines and controlled drugs legislation and where prescribing is in line with NMBI professional regulatory requirements.
Prescriptive authority for controlled drugs is governed by medicines and controlled drugs legislation, including:
- Misuse of Drugs (Amendment) Regulations 2007, specifically Schedule 8, and
- Misuse of Drugs Regulations 2017 (S.I. No. 173/2017)
Schedule 8 sets out the controlled drugs that may be prescribed by nurse and midwife prescribers and the conditions under which prescribing may occur. Only those Schedule 2 MDA medicines listed in Schedule 8 may be prescribed by RNPs or RMPs.
Where medicines or controlled drugs legislation does not provide authority for nurse or midwife prescribing of a particular controlled drug, prescribing is not permitted, even if the registrant is clinically competent or holds NMBI prescriptive authority.
In addition to legislation, prescribing must be carried out in line with NMBI professional standards, including:
You may prescribe Schedule 2 MDA medicines only for individuals you have personally assessed, and only where prescribing is within your individual scope of practice and current competence.
All registrants remain professionally accountable for their prescribing decisions. In accordance with the Code, nurses and midwives must uphold the values of the profession, exercise sound clinical judgement, and ensure that their practice reflects high standards of professional conduct and public protection.
What guidance is provided for the aesthetics industry, specifically in relation to the administration of Botox?
Can a nurse administer medication to patients using a Healthmail prescription?
Yes. A nurse may administer medication based on a valid Healthmail prescription, provided the prescription complies with medicines and controlled drugs legislation and with relevant professional and organisational requirements.
Under the Medicinal Products (Prescription and Control of Supply) (Amendment) Regulations 2020 (S.I. No. 98/2020), the HSE’s Healthmail service is the approved National Electronic Prescription Transfer System. A Healthmail prescription is legally valid where it is transmitted in a permanent, unalterable electronic form and is electronically traceable to the prescriber. It must meet all statutory prescription requirements, including the date of issue and the prescriber’s professional registration number. A handwritten signature is not required, as Healthmail prescriptions are authenticated electronically and must remain in their original, unaltered format.
For Schedule 2 and Schedule 3 controlled drugs, all statutory requirements relating to controlled drug prescriptions continue to apply. While these requirements include specific legal content and format elements, the prescription does not need to be handwritten where it is transmitted through an approved electronic system and is fully traceable to the prescriber. In all cases, the pharmacist must be satisfied that the prescription is legally valid and that dispensing is clinically appropriate within their professional judgement.
A registered nurse may administer medication on foot of a valid Healthmail prescription where the prescription meets legislative requirements and where administration is carried out in accordance with local organisational policies, procedures, protocols, and guidelines (PPPGs).
As with all medication management, you remain accountable for your practice. This includes compliance with the Code of Professional Conduct and Ethics for Registered Nurses and Registered Midwives (NMBI, 2025), Guidance for Registered Nurses and Midwives on Medication Administration (NMBI, 2020), and Guidance to Nurses and Midwives on Medication Management (NMBI, 2007).
These require nurses to apply professional judgement, practise within their individual scope of practice, and ensure that medicines are administered safely and in accordance with applicable legislation.